ON THIS PAGE: You will learn about the different types of treatments doctors use for people with salivary gland cancer. Use the menu to see other pages.
This section explains the types of treatments that are the standard of care for salivary gland cancer. “Standard of care” means the best treatments known. When making treatment plan decisions, you are encouraged to consider clinical trials as an option. A clinical trial is a research study that tests a new approach to treatment. Doctors want to learn whether the new treatment is safe, effective, and possibly better than the standard treatment. Clinical trials can test a new drug, a new combination of standard treatments, or new doses of standard drugs or other treatments. Clinical trials are an option to consider for treatment and care for all stages of cancer. Your doctor can help you consider all your treatment options. Learn more about clinical trials in the About Clinical Trials and Latest Research sections of this guide.
Treatment overview
Many salivary gland cancers can often be cured, especially if found early. Although curing the cancer is the primary goal of treatment, preserving the function of the nearby nerves, organs, and tissues is also very important. When doctors plan treatment, they consider how treatment might affect a person’s quality of life, including how a person feels, looks, talks, eats, and breathes.
In cancer care, different types of doctors often work together to create a person's overall treatment plan that combines different types of treatments. This is called a multidisciplinary team. An evaluation should be done by individual head-and-neck specialists before any treatment begins. The team may include these specialists:
-
Medical oncologist: a doctor who specializes in treating cancer with medication
-
Radiation oncologist: a doctor who specializes in giving radiation therapy to treat cancer
-
Surgical oncologist: a doctor who specializes in treating cancer using surgery
-
Maxillofacial prosthodontist: a specialist who performs restorative surgery in the head and neck areas
-
Otolaryngologist: a doctor who specializes in the ear, nose, and throat
-
Oncologic dentist or oral oncologist: dentists experienced in caring for people with head and neck cancer
-
Physical therapist: a health professional who addresses functional challenges that may develop as a result of cancer and cancer treatment
-
Speech pathologist: a specialist who helps people use muscles in the mouth and throat
-
Mental health providers: health professionals who diagnose and treat mental health problems, such as a psychiatrist or a psychologist
Cancer care teams also include a variety of other health care professionals, such as physician assistants, nurse practitioners, oncology nurses, social workers, pharmacists, counselors, dietitians, and others.
Descriptions of common types of treatments used for salivary gland cancer are listed below. Your care plan also includes treatment for symptoms and side effects, an important part of cancer care.
Take time to learn about all of your treatment options and be sure to ask questions about things that are unclear. Also, talk about the goals of each treatment with your doctor and what you can expect while receiving the treatment. These types of talks are called “shared decision making.” Shared decision making is when you and your doctors work together to choose treatments that fit the goals of your care. Shared decision making is particularly important for salivary gland cancer because there are different treatment options. Learn more about making treatment decisions.
This information is based on the ISOO/MASCC/ASCO guideline, “Management of Salivary Gland Malignancy.” Please note that this link takes you to another ASCO website.
Surgery (updated 04/2021)
Surgery is recommended for nearly everyone diagnosed with salivary gland cancer and is usually the first treatment. During surgery, a doctor performs an operation to remove the cancerous tumor and some surrounding healthy tissue, called a margin. A surgical oncologist is a doctor who specializes in treating cancer using surgery.
The goal of surgery is to remove as much of the tumor as possible and leave negative margins. This means no trace of cancer was found in the healthy tissue that was removed. The type and extent of surgery depends on the location and extent of the cancer.
Types of surgery used to treat salivary gland cancer include:
-
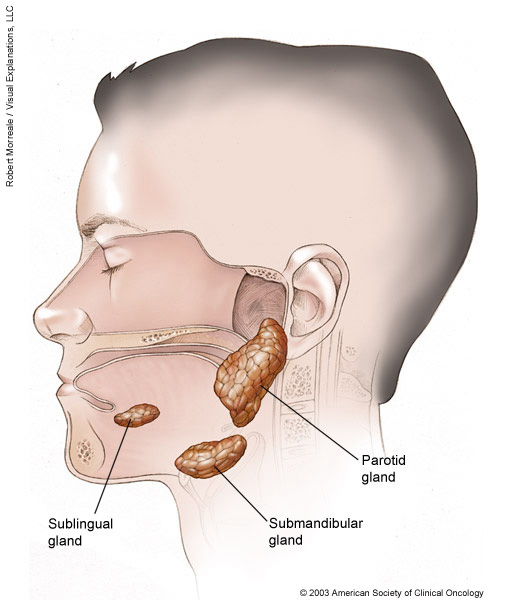
Parotidectomy. Part or all of the parotid gland may be removed during a procedure called a parotidectomy. You have 1 parotid gland on each side of your mouth, located in your cheek and in front of your ear. These are the largest salivary glands in your body. This surgery often involves dissecting the facial nerve. If cancer has spread to the facial nerve, frequently a nerve graft or other reconstructive procedures are necessary for the person to regain use of some facial muscles. Any tissue that is removed can often be restored through reconstructive surgery (see below) and tissue transplantation.
-
Endoscopic surgery. Occasionally, it is possible to remove the tumor by endoscopic surgery (see Endoscopy, under Diagnosis), which is less destructive to healthy tissues than regular surgery. This is used particularly when a salivary gland tumor begins in the paranasal area (around the nose) or in the larynx. However, this is rare. More often, a tumor may be found unexpectedly during endoscopic surgery for what is believed to be chronic sinusitis (inflammation).
-
Neck dissection. A neck dissection is when the surgeon examines all of the critical structures in the neck and removes lymph nodes from the neck. This may be performed if the doctor suspects that the cancer has spread, or if there is a high enough chance of it spreading. A neck dissection may cause numbness of the ear, weakness when raising the arm above the head, and weakness of the lower lip. These side effects are caused by injury to nerves in the area. Depending on the type of neck dissection, weakness of the lower lip and arm may go away in a few months. Weakness will be permanent if a nerve is removed as part of the dissection.
-
Reconstructive surgery. Reconstructive (plastic) surgery may be used to replace tissue and nerves that were removed during surgery to eliminate the cancer.
Surgery can have significant risks because the cancer may be close to the eyes, mouth, brain, and important nerves and blood vessels. Surgical side effects can include swelling of the face, mouth, and throat, which makes it difficult to breathe and swallow. Frequently, a person may receive a temporary tracheostomy, a hole in the windpipe, to make breathing easier during their recovery.
Facial nerves may also be affected, either temporarily or permanently, by cancer or its treatment. Whenever possible, the surgeon will try to preserve function of the facial nerves. Changes to a person’s appearance because of surgery may need to be addressed using reconstructive plastic surgery. If the maxilla (upper jaw) is removed, a prosthodontist will play a large role in the rehabilitation process. A prosthodontist is a dentist who specializes in replacing teeth and parts of the jaw. Learn more about cancer rehabilitation.
Surgery is typically followed by additional treatment, most often radiation therapy. Sometimes, more than 1 operation may be needed to remove the cancer and to help restore the appearance and function of the affected tissues. If the cancer comes back after surgery, then additional surgery or other treatment may be recommended. Occasionally, it is not possible to remove salivary gland cancer using surgery. This type of tumor is called inoperable. In these cases, doctors will recommend other treatment options (see below).
Before surgery, talk with your health care team about the possible side effects from the specific surgery you will have. Learn more about the basics of cancer surgery.
Radiation therapy (updated 04/2021)
Radiation therapy is the use of high-energy x-rays or other particles to destroy cancer cells. A doctor who specializes in giving radiation therapy to treat cancer is called a radiation oncologist. A radiation therapy regimen, or schedule, usually consists of a specific number of treatments given over a set period of time.
For a salivary gland tumor, radiation therapy is most often used in combination with surgery. Whether radiation therapy is given after surgery depends on the size, grade, extent, and location of the cancer and whether there are some cancer cells in the margin around the tumor removed by surgery. If radiation therapy is recommended, it should be started within 8 weeks of the surgery. Radiation therapy may also be given along with chemotherapy (see below). If a person cannot have surgery or decides not to have surgery, radiation therapy may be used as the main treatment.
There are 2 main types of radiation therapy used for salivary gland cancer:
-
External-beam radiation therapy. This is the most common type of radiation treatment and is given from a machine outside the body. External-beam radiation therapy may be used when a tumor has grown into the soft tissue, has spread to the lymph nodes, surrounds a nerve, or when surgery is not possible. Doctors also recommend this type of radiation therapy for poorly differentiated tumors. (See the Stages and Grades section for more information.)
A specific method of external radiation therapy, known as intensity modulated radiation therapy (IMRT), allows more effective doses of radiation therapy to be delivered while reducing damage to nearby healthy cells.
Other types of external-beam radiation therapy used for salivary gland tumors are proton, neutron, and carbon ion therapy. These types of radiation therapy use particles other than x-rays.
- Internal radiation therapy. When radiation therapy is given using implants, it is called internal radiation therapy or brachytherapy. Internal radiation therapy involves surgically implanting tiny pellets or rods containing radioactive materials in or near the tumor.
Before beginning radiation treatment for salivary gland cancer, a person should receive a thorough examination from an oncologic dentist or oral oncologist. These doctors are experienced in treating people with head and neck cancer. Radiation therapy can cause tooth decay. Often, tooth decay can be prevented with proper treatment from a dentist before beginning treatment. Learn more about dental and oral health.
Other side effects from radiation therapy to the head and neck may include redness or skin irritation in the treated area, dry mouth (xerostomia) or thickened saliva from damage to salivary glands, bone pain, nausea, fatigue, mouth sores, and/or sore throat. People may also experience pain or difficulty swallowing; loss of appetite, often due to a change in sense of taste; hearing loss, due to the buildup of fluid in the middle ear; and buildup of earwax that dries out because of the radiation therapy’s effect on the ear canal.
Radiation therapy may also cause a condition called hypothyroidism in which the thyroid gland (located in the neck) slows down and causes the person to feel tired and sluggish. People who receive radiation therapy to the neck area should have their thyroid checked regularly. Talk with your health care team about what side effects of your treatment plan are possible and how they can be prevented or managed.
Learn more about the basics of radiation therapy.
Therapies using medication (updated 12/2022)
The treatment plan may include medications to destroy cancer cells. Medication may be given through the bloodstream to reach cancer cells throughout the body. When a drug is given this way, it is called systemic therapy. Medication may also be given locally, which is when the medication is applied directly to the cancer or kept in a single part of the body.
This treatment is generally prescribed by a medical oncologist, a doctor who specializes in treating cancer with medication. Research continues about the benefits of systemic therapy to treat salivary gland cancer, and this type of treatment is being evaluated in clinical trials.
For salivary gland cancer, therapies using medication are most often used to treat later-stage cancer or to relieve symptoms. Some drugs are available in clinical trials that may treat cancer at an earlier stage or that may be combined with radiation therapy to determine its effectiveness.
When medication is recommended, the main type is chemotherapy. Chemotherapy is the use of drugs to destroy cancer cells, usually by keeping the cancer cells from growing, dividing, and making more cells.
A medication called targeted therapy may be an option through clinical trials for people with certain subtypes of salivary gland cancer if the tumor has specific genetic changes or molecular alterations, including HER2, NTRK, or androgen receptors.
If the tumor has high tumor mutational burden (TMB) or expresses a protein called PD-L1, then treatment using pembrolizumab (Keytruda) may be recommended. Pembrolizumab is a type of medication called immunotherapy. Immunotherapy uses the body's natural defenses to fight cancer by improving your immune system's ability to attack cancer cells.
Medication gets into the bloodstream to reach cancer cells throughout the body. Common ways to give cancer medications include an intravenous (IV) tube placed into a vein using a needle or in a pill or capsule that is swallowed (orally). If you are given oral medications, be sure to ask your health care team how to safely store and handle them.
A regimen, or schedule, usually consists of a specific number of cycles given over a set period of time. A person may receive 1 drug at a time or a combination of different drugs given at the same time.
Each drug or combination of drugs can cause specific side effects, and it is important to talk with your doctor about which side effects to expect and whether any may be permanent. The side effects of systemic therapy depend on the individual and the dose used, but they can include fatigue, risk of infection, nausea and vomiting, hair loss, loss of appetite, diarrhea, and open sores in the mouth. Talk with your health care team about how they can help manage or relieve treatment side effects.
The medications used to treat cancer are continually being evaluated. Talking with your doctor is often the best way to learn about the medications prescribed for you, their purpose, and their potential side effects or interactions with other medications. It is also important to let your doctor know if you are taking any other prescription or over-the-counter medications or supplements. Herbs, supplements, and other drugs can interact with cancer medications, causing unwanted side effects or reduced effectiveness. Learn more about your prescriptions by using searchable drug databases.
This information is based in part on the ASCO guideline, “Immunotherapy and Biomarker Testing in Recurrent and Metastatic Head and Neck Cancers.” Please note that this link takes you to a different ASCO website.
Physical, emotional, and social effects of cancer
Cancer and its treatment cause physical symptoms and side effects, as well as emotional, social, and financial effects. Managing all of these effects is called palliative care or supportive care. It is an important part of your care that is included along with treatments intended to slow, stop, or eliminate the cancer.
Palliative care focuses on improving how you feel during treatment by managing symptoms and supporting patients and their families with other, non-medical needs. Any person, regardless of age or type and stage of cancer, may receive this type of care. And it often works best when it is started right after a cancer diagnosis. People who receive palliative care along with treatment for the cancer often have less severe symptoms, better quality of life, and report that they are more satisfied with treatment.
Palliative treatments vary widely and often include medication, nutritional changes, relaxation techniques, emotional and spiritual support, and other therapies. You may also receive palliative treatments similar to those meant to get rid of the cancer, such as chemotherapy, surgery, or radiation therapy.
Before treatment begins, talk with your child’s doctor about the goals of each treatment in the treatment plan. You should also talk about the possible side effects of the specific treatment plan and palliative care options.
During treatment, your health care team may ask you to answer questions about your/your child’s symptoms and side effects and to describe each problem. Be sure to tell the health care team if you are experiencing a problem. This helps the health care team treat any symptoms and side effects as quickly as possible. It can also help prevent more serious problems in the future.
Learn more about the importance of tracking side effects in another part of this guide. Learn more about palliative care in a separate section of this website.
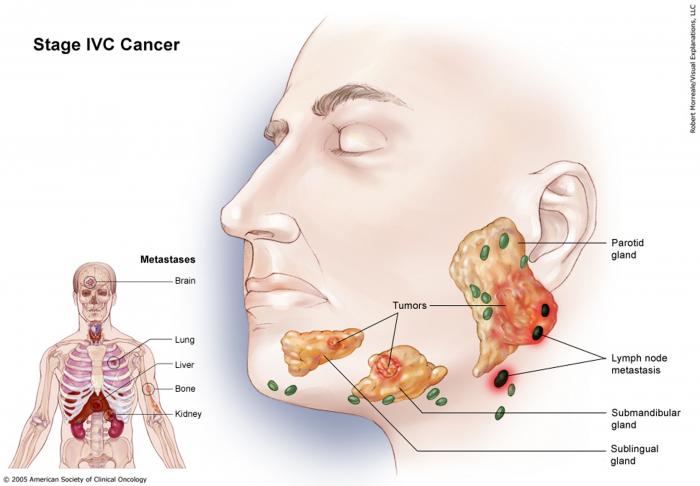
Metastatic salivary gland cancer (updated 04/2021)
If cancer spreads to another part in the body from where it started, doctors call it metastatic cancer. If this happens, it is a good idea to talk with doctors who have experience in treating it. Doctors can have different opinions about the best standard treatment plan.
Not all salivary gland cancers behave in the same way, and for some very slow-growing cancers, your doctor may recommend observation. Clinical trials might also be an option. Learn more about getting a second opinion before starting treatment, so you are comfortable with your chosen treatment plan.
Your treatment plan may include 1 or more of the treatments listed above, depending on the subtype of the salivary gland cancer, the extent of the disease, and your symptoms. Typically, the main treatment is standard chemotherapy or targeted therapy, especially if a specific tumor marker such as HER2 or NTRK is found in your tumor (see above). Some of treatment options may be available by taking part in a clinical trial. Your doctor may also recommend further testing to determine the specific characteristics of your cancer. If certain tumor alterations are found, targeted therapy or another type of systemic therapy called immunotherapy (see Latest Research) may be options. Palliative care will also be important to help relieve symptoms and side effects.
For most people, a diagnosis of metastatic cancer is very stressful and difficult. You and your family are encouraged to talk about how you feel with doctors, nurses, social workers, or other members of the health care team. It may also be helpful to talk with other people with cancer, including through a support group.
Remission and the chance of recurrence
A remission is when cancer cannot be detected in the body and there are no symptoms. This may also be called having “no evidence of disease” or NED.
A remission may be temporary or permanent. This uncertainty causes many people to worry that the cancer will come back. While many remissions are permanent, it is important to talk with your doctor about the possibility of the cancer returning. Understanding your risk of recurrence and the treatment options may help you feel more prepared if the cancer does return. Learn more about coping with the fear of recurrence.
If the cancer returns after the original treatment, it is called recurrent cancer. It may come back in the same place (called a local recurrence), nearby (regional recurrence), or in another place (distant recurrence).
When this occurs, a new cycle of testing will begin again to learn as much as possible about the recurrence. After this testing is done, you and your doctor will talk about the treatment options. Often the treatment plan will include the treatments described above, such as surgery, radiation therapy, or chemotherapy, but they may be used in a different combination or given at a different pace. Your doctor may suggest clinical trials that are studying new ways to treat this type of recurrent cancer. Whichever treatment plan you choose, palliative care will be important for relieving symptoms and side effects.
People with recurrent cancer often experience emotions such as disbelief or fear. You are encouraged to talk with the health care team about these feelings and ask about support services to help you cope. Learn more about dealing with cancer recurrence.
If treatment does not work
Recovery from cancer is not always possible. If the cancer cannot be cured or controlled, the disease may be called advanced or terminal.
This diagnosis is stressful, and for many people, advanced cancer may be difficult to discuss. However, it is important to have open and honest conversations with your health care team to express your feelings, preferences, and concerns. The health care team has special skills, experience, and knowledge to support patients and their families and is there to help. Making sure a person is physically comfortable, free from pain, and emotionally supported is extremely important.
People who have advanced cancer and who are expected to live less than 6 months may want to consider hospice care. Hospice care is designed to provide the best possible quality of life for people who are near the end of life. You and your family are encouraged to talk with the health care team about hospice care options, which include hospice care at home, a special hospice center, or other health care locations. Nursing care and special equipment can make staying at home a workable option for many families. Learn more about advanced cancer care planning.
After the death of a loved one, many people need support to help them cope with the loss. Learn more about grief and loss.
The next section in this guide is About Clinical Trials. It offers more information about research studies that are focused on finding better ways to care for people with cancer. Use the menu to choose a different section to read in this guide.